Why Women in Menopause Are Adding This Easy Fix to Their Nightly Routine
Even after magnesium, HRT, and sleep hygiene, 1 in 2 menopausal women still wake at 4 AM.¹

Let's talk about something no menopausal woman gets warned about.
Not the HRT. Not the magnesium. Not the sleep hygiene. Those are working.
By 47, that part of the stack is finally doing its job. The hot flashes softened. The mood stabilised. Some symptoms lifted.
Some didn't.
The 4 AM wakings, heart pounding for no reason. The brain fog at 2.30. The exhaustion no weekend ever quite fixes.
51.6% of menopausal women have a sleep disorder, even with a properly layered stack.¹
One that has almost nothing to do with the hormones the stack already addresses.
Almost everything to do with something physical. Something mechanical. Something fixable.
Here's what we found.
But first: what the menopause stack quietly misses.
Sleep researchers have measured something surprising. Only 27% of nighttime wake time in menopausal women is directly attributed to hot flashes.⁹
The other 73% is something else.
Most of it points at neurology. Temperature regulation. Stress response. Estrogen and progesterone decline disrupting multiple systems at once.
All real. None of it complete.
For many menopausal women, there's one more layer underneath. A mechanical one.
Not in the bloodstream. Not in the hormonal axis. Not in any place a supplement was ever designed to reach.
After perimenopause, falling oestrogen weakens the collagen scaffolding that holds soft tissue in place across the body.²
The same mechanism that affects bone density, cartilage, and connective tissue everywhere else.
Including, for many women, one specific 2cm flap of cartilage at the top of the nose. Called the nasal valve.
The narrowest part of your airway. The first part that has to stay open for you to sleep without effort.
Think of your hormones as the support system for your airway. When that support fades, the soft tissue around the valve can sag just enough to interfere with breathing at night.
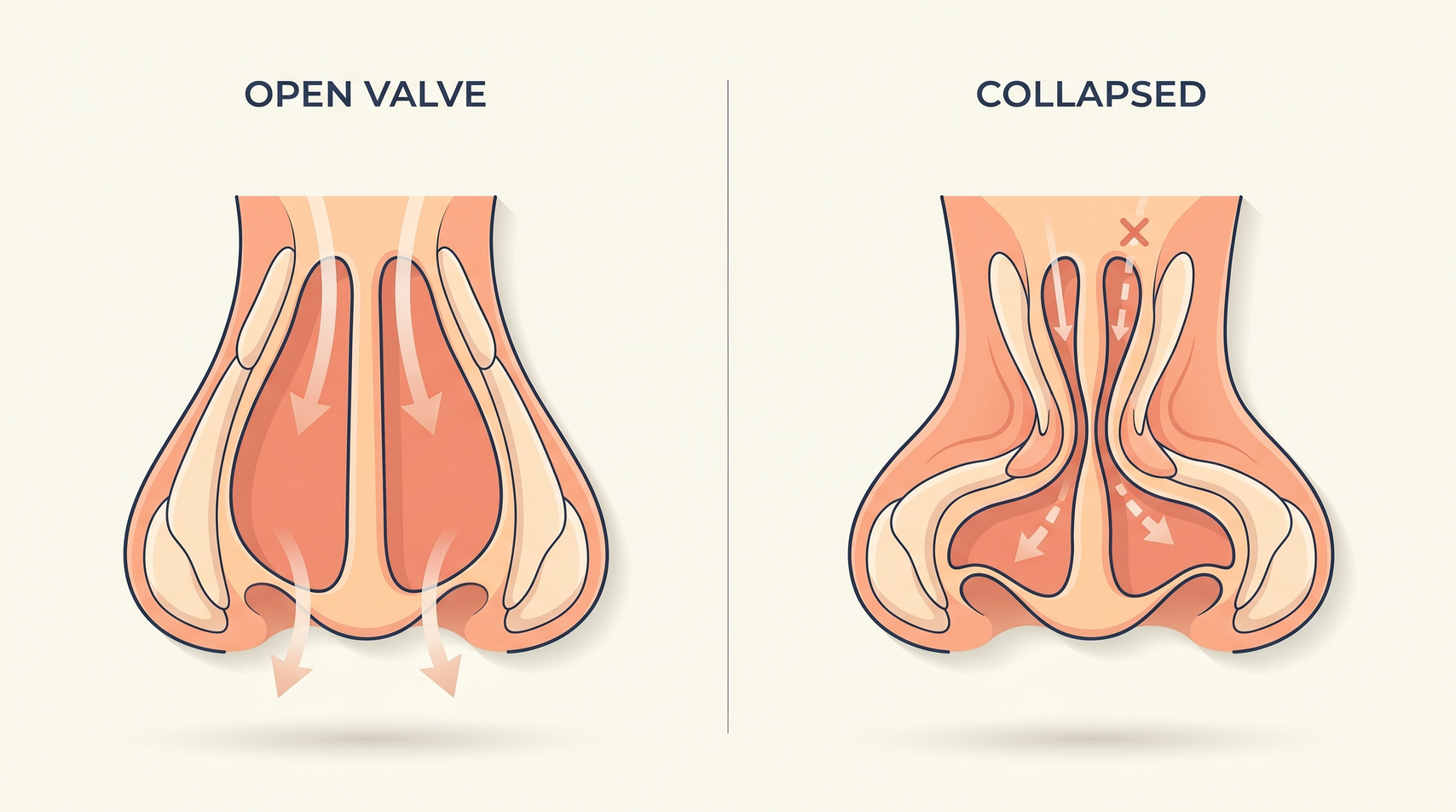
When the valve weakens, it collapses slightly during the negative-pressure phase of inhalation. The body compensates by opening the mouth. And the breathing pattern shifts, silently, from nasal to oral, all night, every night.
That can be one real cause of fragmented sleep after perimenopause.
Not the loud snoring most women never even do.
Not the hormonal shift on its own.
A 2cm valve, weakened by falling oestrogen, collapsing quietly every time you lie down.
Which means part of what stayed broken, even with everything else working, may have had a mechanical cause all along.
See if this quick fix solves it for you. Test tonight, in your own bed.
Check AvailabilitySo what does all this mean for the way you've been feeling?
This isn't a personal failing.
It's a mechanical layer the stack can't reach.
The brain fog at 2.30 in the afternoon isn't a memory problem.
The 4 AM waking with your heart pounding isn't anxiety you can think your way out of.
The exhaustion no weekend ever quite fixes isn't a sign you're "doing too much."
They're all the same thing.
A sleep architecture fragmenting, night after night, because a 2cm valve fails in the dark.
Not the hormones working alone. Not your stress. Not a discipline you let slip.
The collagen around your airway weakens the same way it does throughout the body after perimenopause.
And the consequences land where you feel them. In your sleep. Your focus. Your patience. Your edge.
Once you see it as a mechanical problem, the whole picture shifts.
You haven't been losing yourself. You've been losing your nights, one collapsed valve at a time.
So why hasn't anyone made the connection for you?
Because your symptoms already have a name on them.
Brain fog. Broken sleep. Exhaustion. The 4 AM wakings.
At your age, every clinical guideline puts those under menopause. And every clinical guideline is right. Just not complete.
Which is why your GP follows the menopause map. HRT first. Then melatonin, or an antidepressant if sleep doesn't improve.
Each step rational. None of it pointing at a 2cm flap of cartilage.
Other specialists could see this. But you only get sent to them when there's loud snoring or a drop in oxygen on a sleep study. Not "I keep waking at 4 AM with brain fog."
The connection itself is new. It hasn't yet entered routine training. It will.
But not before another generation of women has been told the same thing, in different rooms, by different doctors.
On average, this gap goes unaddressed for eight years.
Eight years the stack runs exactly as designed on the hormonal side.
Eight years the mechanical side keeps fragmenting the sleep underneath.
The Signals Your Stack Wasn't Designed to Catch
If you recognise three or more of these, you are not imagining the pattern. You are looking at it.
- You wake up with a bone-dry mouth, most mornings, no matter how much water you drank the night before.
- Your partner has mentioned, more than once, that you breathe loudly at night. You don't think of yourself as a snorer.
- If you wear a sleep tracker, the pattern is right there: low deep sleep, low REM, frequent wakings you can't remember.
- Your throat is sore in the morning. Or your tongue has ridges along the edges when you look in the mirror.
- You wake at 4 am with your heart pounding for no reason, several nights a week.
- The brain fog rolls in like a curtain around 2.30 in the afternoon, even on the days you slept 'well'.
- Hot flashes that wake you, or night sweats that soak the sheets.
- Tired but wired: exhausted, but unable to shut your mind off at midnight.
Yes, the research is already there
Take all five signals together and you find a pattern researchers have been mapping for a decade.
Postmenopausal women have a 2 to 3 times higher rate of sleep apnoea than women before menopause. And it almost never shows up the way the textbook describes it. Insomnia, fatigue, mood swings, rather than loud snoring.⁵
Behind that, an even older finding: 70 to 95% of women who develop the more serious form of sleep apnoea began as habitual, quiet snorers. The airway closes long before anyone names what is happening.⁴
The brief wakings nobody can remember in the morning are not random. They correlate directly with how restricted the airway is at night.⁶
Mouth-breathing through that restriction is linked to measurable next-day cognitive decline. Memory. Focus. The words that should be there at 2.30 pm.⁷
And the cost of leaving it unaddressed isn't just brain fog. Women with poor sleep quality during menopause are three times more likely to score poorly on cardiovascular health measures. The American Heart Association now counts sleep as one of the eight key measures of heart health.⁸
On the mechanical side, the science is just as clear. Supporting the nasal valve from the outside drops airway resistance by 21 to 39% in clinical tests.³
None of it is theory. All of it is in the journals.
The layer your menopause stack can't reach
If you're reading this, you probably already have a stack.
Your HRT, at the right dose. Your magnesium glycinate at night. Your L-theanine for the racing thoughts. Your melatonin, timed two to three hours before bed. Your sleep hygiene protocol from the latest research.
All of it is doing real work on the hormone layer.
None of it is doing anything for a 2cm flap of cartilage.
Because supplements and HRT both work biochemically. They cross into the bloodstream. They balance hormones. They calm cortisol. They sometimes nudge sleep.
They do not, and cannot, hold a piece of soft tissue in place from the outside.
That requires a different kind of intervention. A mechanical one.

The category exists. It's called external nasal valve support.
The idea is simple: hold the 2cm flap open at night, from the outside, so the airway stays open without effort.
ClearStrip is one of these. An external nasal valve support, made for adults to use at home.
It sits across the bridge of the nose at night, gently lifting the 2cm flap from the outside.
Drug-free. Reversible. No prescription. No diagnosis required.
It is not a menopause product. It is a structural one.
For any adult whose nighttime airway is narrowed by soft-tissue change. Many of those adults happen to be perimenopausal women.
Your supplements, your sleep hygiene, your routines work alongside it.
They've never been the wrong answer for the hormonal side. They were just never going to reach the mechanical side.
This isn't a replacement for any of them. It's the layer underneath them, the one your stack couldn't get to.
And it's the first thing you can try, before any of the bigger ones.
The four steps, from smallest to biggest
There are four ways to support an airway that collapses at night. Each one is bigger than the last.
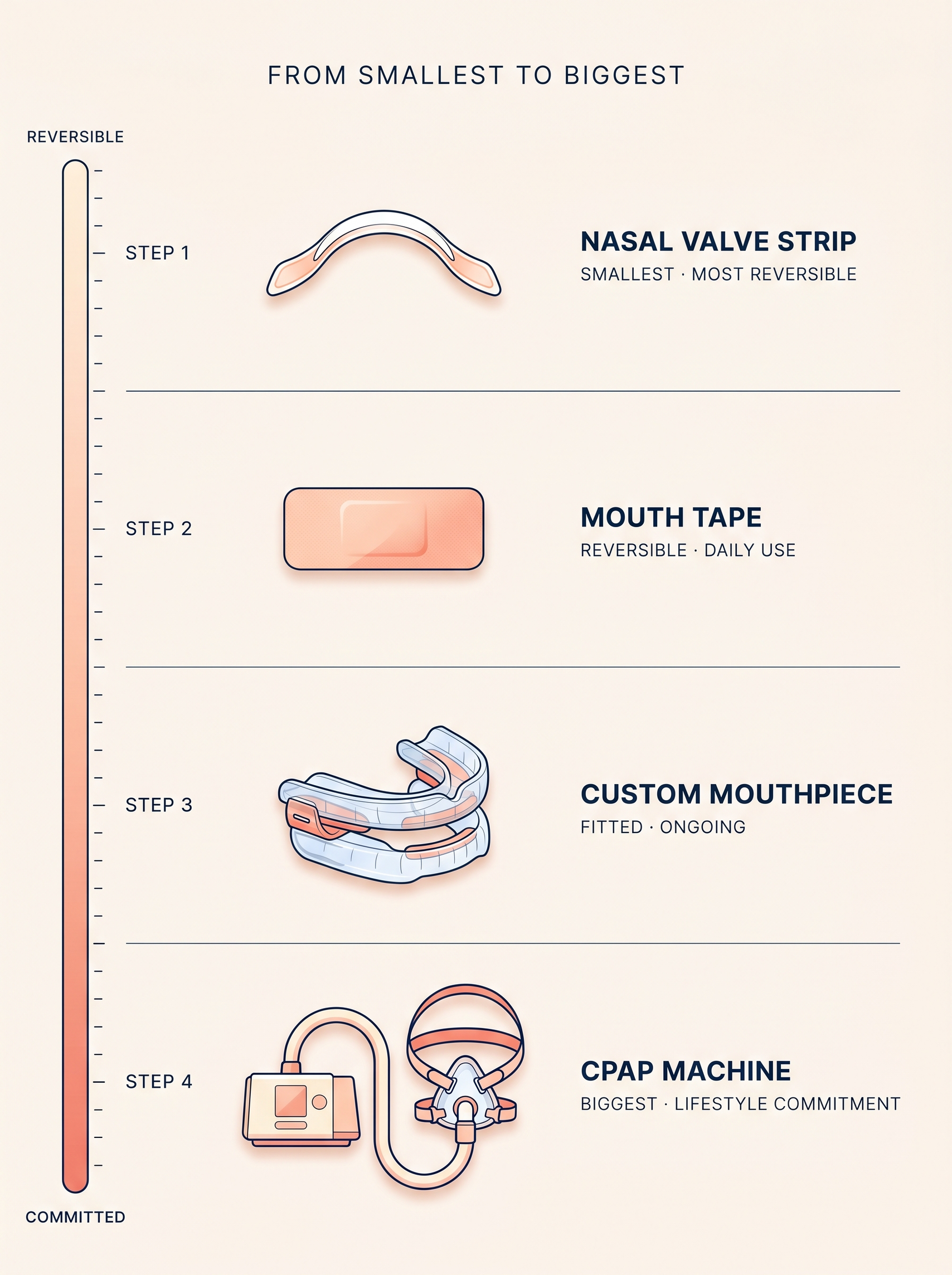
The first is an external nasal valve support, like ClearStrip. Worn across the bridge of the nose. Five seconds on, five seconds off.
The second is mouth tape or an internal nasal dilator. Mainly marketed to athletes. Many women find them uncomfortable.
The third is a custom mouthpiece that shifts your jaw forward at night. Dental fitting, around £200 to £500. Some people adjust. Some don't.
The fourth is a sleep clinic study followed by a CPAP machine. A mask and pressurised air, every night. A lifestyle commitment.
Most women dealing with menopause-attributed sleep loss skip the first option entirely. Not because it doesn't work for them. Because no one shows it to them.
Which means they end up considering option three or four, when option one was the obvious place to start.
The first is the smallest thing you can try. It's also the most reversible. If it doesn't work, the other three are still there. In the order you'd take them.
And you can't know if you need the bigger ones until the smallest one has been tried.
For the women who refused to call broken sleep just menopause.
Check AvailabilityNight 1 to Day 90: what to look for
Here's what to look for, night by night, if it's working for you.
Night 1. You wake up with a moist mouth instead of a dry one. The airway stayed open.
Week 1. Your sleep tracker, if you wear one, shows more time in deep sleep. Fewer of those brief wakings you couldn't remember.
Month 1. The brain fog at 2.30 in the afternoon is softer. Energy more reliable. Sleep starts to feel restorative, the way you remember it.
Day 90. Someone close to you notices you look different. You don't tell them, at first, what you changed.
You keep your supplements. You keep your sleep routine.
You add a 5-second mechanical fix that those were never designed to reach.
Not every woman has this experience.
Some find their sleep improves immediately. Some need a week of nights for the body to settle into the new pattern. Some discover, after honestly trying, that they need to climb to the bigger steps after all.
And starting at the smallest step means you'll know within weeks, not years.
Not a purchase. A test.
Five seconds at bedtime. No prescription.
Free UK shipping.
The smallest thing to try first.
Sources
Shafie M et al. (2023). Global prevalence of sleep disorders during menopause: a meta-analysis. PMC9996569. View study.
Estrogen decline and soft tissue laxity in postmenopausal women. Peer-reviewed literature.
Gehring W et al. (2019). Effect of external nasal dilators on nasal airway resistance. PMC6822853. View study.
Pevernagie D et al. (2009). Sleep apnoea progression from habitual snoring. European Respiratory Journal.
Mirza M, Lal D et al. Obstructive sleep apnoea in postmenopausal women: prevalence and atypical presentation. Sleep Medicine.
Polysomnography meta-analysis: nasal airway resistance and micro-arousals during sleep.
Chronic mouth-breathing during sleep and daytime cognitive impairment. Peer-reviewed literature.
Aggarwal B et al. (2023). Sleep problems linked to heart health risks during and after menopause. American Heart Association / Circulation: Cardiovascular Quality and Outcomes.
de Zambotti M, et al. (2018). Sleep and sleep disorders in the menopausal transition. PMC6092036. View study.
Comments (3)
I was skeptical, honestly. I already do magnesium glycinate, L-theanine, the whole sleep ritual, blackout curtains, blue-light glasses, the works. Adding one more thing felt redundant. But the 3 AM wakings kept coming back. Tried this for two weeks. First few nights I noticed the morning dry mouth was just gone. By week two my tracker showed an extra 40 minutes of deep sleep. Same routine. One small mechanical change.
I never write reviews but I have to say something. I've been waking up at 3-4 AM for almost ten years. HRT helped some, but the broken sleep stayed. Tried this for about a month. The morning dry mouth started easing around week two. The wakings have become less frequent, not gone. For me, less frequent after ten years is already a big shift.
Ten years of trying everything I could think of. Magnesium glycinate, melatonin, blackout curtains, white noise, the whole bedtime ritual. Some of it helped a little, none of it fixed the 3 AM wakings. A friend mentioned this and I thought, fine, one more thing. After a couple of months I noticed I was sleeping through more often than not. Not perfect, but more than I'd say about anything else I'd tried.
Leave a comment
Thank you for your comment
We will review it as soon as possible.